Since the World Health Organization announced the Corona Pandemic in March 2020, the world has faced many challenges and fundamental lifestyle changes. This study aims to identify lifestyle changes such as diet, marketing habits, daily activities, and sleep patterns in the western region of Saudi Arabia (SA) during the COVID-19 quarantine period. Besides, this work aims to investigate the relationship between lifestyle changes and weight changes. A retrospective cross-sectional study conducted in the western region, SA during the COVID -19 quarantine between May 2020 and January 2021. The descriptive research approach was adopted using a questionnaire. Subjects who met the admission requirements and completed the questionnaire was 539. The majority of participants’ ages 35-44 years, they were mainly women (73.3%). The percentage of those who work from home (online) was 31.2%. Most respondents rely on home-cooked food during the quarantine period (84 %), and the proportion of people eating out at restaurants is declining. About half of the participants reported emotional eating (54 %), and the majority preferred sweets. 42.4% of participants did not store additional food or worry about food insecurity. 44 % of participants revealed weight gain. There were strong correlation between increased weight in the study participants and emotional eating (p < 0.001), physical exercise (p < 0.001), and the number of fast-food consumed per week (p< 0.05). This work showed that weight gain in people during the lockout period could be attributed to the reduction in exercise and physical activity and the increased in emotional eating.
INTRODUCTION
Coronavirus ailment has been a general health crisis of international worry since January 2020 (WHO, 2020a). The food sector had faced diverse challenges throughout the pandemic. Food sustainability, security, and safety are strongly affected dimensions of food systems during the COVID-19 quarantine. The COVID-19 has obligatory the Saudi government to impose hygiene restrictions to prevent or reduce infection (Galanakis et al., 2020). Also, there were national lockdown measures, and public gathering places as shopping malls and restaurants were closed (Ruiz-Roso et al., 2020). In April 2020, the Saudi government obligatory a total curfew that allowed people to leave their homes only at a limited time (Obeid et al., 2020). Besides, the negative consequence of quarantine, also called self-quarantine, on health and socioeconomic status (Vieira et al., 2020), also anxiety, stress, boredom, depression, limited physical activity, emotional eating, and sleep disorders have been documented during quarantine (Bhutani & Cooper, 2020; Sidor & Rzymski, 2020; Bakhsh et al., 2021).
Nutritional status has been severely changed during the quarantine and the pandemic (Scarmozzino & Visioli, 2020; Sidor & Rzymski, 2020). Research proved the association between boredom and changing dietary lifestyle habits through higher eating of high energy, fat, carbohydrate, and protein foods and unhealthy eating behavior, and weight changes (Alzahrani et al., 2020; Muscogiuri et al., 2020). Moreover, stress has a direct impact on dietary habits. In social isolation, people are put under psychological stress, which makes them overeat in response to emotional triggers (Reyes-Olavarría et al., 2020; He et al., 2021). The COVID-19 lockdown influences lifestyle habits by increasing consumption of foods, excessive food storage, and decreasing physical activity (Di Renzo et al., 2020; Park et al., 2020). Additionally, staying for a long time at home, especially with distance learning and working online, increases the use of screen-based time activities that impact bad eating habits (Pokhrel & Chhetri, 2021).
Galli et al. (2020) demonstrated that the COVID-19 quarantine imposed unique lifestyle resulted in a circadian misalignment, which can induce eating behaviors changes and body weight gain, in reaction to mental stress, sedentary lifestyle, spending more time at home, and improve visual and olfactory stimulation to eat. Circadian rhythms counterpart most biological processes as hormonal secretion, metabolism, and gastrointestinal functions (Patton & Hastings, 2018). Besides, peoples’ lifestyles were changed during self-quarantine, shopping for fresh groceries became complicated. Storage of food products due to fear of shortages of certain food products might happen, causing disruptions in the food chain around the country (Calder et al., 2020; Jansen et al., 2020; Parmet & Sinha, 2020). These changes produce adaptive and compensatory responses that could last for months and even for generations, thus requiring more attention to restore the dysregulated metabolic processes (Maggini et al., 2018).
In addition, there was a significant decline in physical activity in populations during quarantine relative to WHO recommendation for healthy adults (150 min. of moderate activity weekly or 75 min. of strongly activity weekly) (WHO, 2020b). Recently Bakhsh et al. (2021) documented that COVID-19 harmed physical activity which was related to significant weight gain.
Limited information is available on the effect of quarantine on life modification and its impact on body weight in the western region, Saudi Arabia. Therefore, the current study aimed to determine lifestyle changes, including eating behaviors, marketing habits, daily activities, and sleep behavior in the western region, Saudi Arabia, during the COVID-19 quarantine time. Also, to explore the relationship between modification on lifestyle and the variations in body weight.
MATERIALS AND METHODS
Study Design and Sample Size
This study is a retrospective cross-sectional study. It was conducted in Saudi Arabia from May 2020 to January 2021. The least number of subjects involved in this questionnaire was 384 individuals to reach a 5% margin of error and a 95% confidence limit. Seven hundred forty-eight subjects filled the survey, but only 539 members met the inclusion requirements the total number of members who met the inclusion requirements was 539.
Inclusion and Exclusion Criteria
All participants should be Saudi citizens from the western region, both gender, educated, and over 15. Any samples which not meet the inclusion criteria were excluded from this study.
Data Collection
The descriptive research approach was adopted using an electronic questionnaire, which was translated into Arabic. The Google form questionnaire’s link was sent to the participants via social networks. Every participant should only send one reply. Replies of participants were double-checked to emphasize that no reply was duplicated.
The questionnaire includes four types of questions. The first section comprises demographic and social characteristics of the study population such as age, gender, education level, social status, number of children, health status, and work status. The second section assesses nutritional habits and bodyweight variation of the study population during the COVID-19 pandemic, such as the amount of water consumed, number of meals, reasons for skipping some daily meals, types of meals, reasons for not eating in restaurants, number of fast-food meals, emotional eating, types of food most common in persons experienced emotional eating, and body weight variation during the COVID-19 pandemic. The third section inquiries marketing habits of the study population during the COVID-19 pandemic such as storing extra amounts of food, online food shopping, sterilization of the purchased foods, and changing in meat purchase habits. Finally, the fourth section examines daily activities and sleep habits of the study population during the COVID-19 pandemic, such as hours of work or study per day, the number of doing house cleaning per week, days of physical exercise per week, hours of daily entertainment, hours of sleep per day, sleep quality, experience anxiety as a result of the pandemic, and energy level during the day. Survey validity was checked beforehand. The survey was given to five faculty staff, King Abdulaziz University, who were asked to rate each item on a 5-point Likert scale ranging from 1 to 5 (1=strongly important, 2 = important, 3 = neither important nor not important, 4= not important, and 5 = strongly not important). There was an excellent item-content validity index.
Statistical Calculations
The acquired results were descriptively analyzed. Frequency (percentages and/or counts) is used to represent the replies. A chi-squared test was used for data analysis. Prism® was used to perform statistical analysis on the results (version 8.4.0, GraphPad Software Inc., La Jolla, CA, USA). The significance level was settled as P ≤ 0.05.
RESULTS AND DISCUSSION
Demographic and Social Characteristics of the Participants
This study included 539 participants aged from 15 years to more than 55 years; most of them (39%) lie between 35-44 years, while only 7.1% of them aged between 55 years and more. Most of the participants were females (73.3%) compared to 26.7% males. Most of the participants were university-educated (59.2%), 73.8 % of them were married, most of them had 3 or more children (48.4%). The majority of the participants were healthy (74 %), and the percentage of those who work from home (online) was 31.2%, while 34.7% of the participants were those who go to workplaces (Table 1).
Nutritional Habits and Bodyweight Variation of the Participants during the COVID-19 Pandemic
From the data obtained, 56.2% of the participants consumed 1-4 glasses of water daily, 27.5% consumed 5-7 glasses, and only 16.3% consumed 8 or more glasses. Nearly half of the participants (50.8%) consume 1-2 meals per day, while 46.4% eat 3-4 meals. Approximately 88.1% of the individuals skipped some daily meals on a regular or irregular basis. The following were the main reasons for skipping some meals: lack of time (37.3%), weight loss (24.3%), loss of appetite (18.7%), a drop in daily food consumption (16.7%), and fasting (3%) are all factors. According to the findings, 84% of the participants rely on home-cooked meals, while the percentage of people who eat out has dropped to 14.3%. Outside of the home, there is a wide range of dining options, including restaurants (9.3%), fast food (4.5%), and restaurants serving healthy meals (0.5%). The lack of consumption of restaurants food at 27.1% of the participants is due to their desire to focus on healthy food that raises immunity. While 22.5% justified their lack of eating in restaurants for fear of pollution, 17.6% were due to the low nutritional value, and the high price was the justification for 32.8% of the participants. The percentage of people who consume fast food has declined, with 13.2% saying they don’t eat fast food at all and 63.3% saying they eat it once or twice a week. Emotional ingestion was found in 54% of the participants, with 44.3% percent preferring sugars, 28.1% chips and biscuits, 13.7% pastries, and 13.9% nuts. During the pandemic’s quarantine period, 44% of participants reported a rise in body weight. In 38% of the participants, bodyweight stayed unchanged, while just 18% lost weight (Table 2).
Table 1. Demographic and social information of the participants (n=539)
|
Character |
Frequency (%) |
|
Sex |
|
|
Male |
144 (26.7%) |
|
Female |
395 (73.3%)# |
|
Age (year) |
|
|
15-24 |
67 (12.4%) |
|
25-34 |
121 (22.4%) |
|
35-44 |
210 (39.0%)# |
|
45-54 |
103 (19.1%) |
|
> 55 |
38 (7.1%) |
|
Education level |
|
|
Pre-university |
140 (26.0%) |
|
University |
319 (59.2%)# |
|
Postgraduate |
80 (14.8%) |
|
Social status |
|
|
Single |
114 (21.2%) |
|
Married |
398 (73.8%)# |
|
Divorced |
19 (3.5%) |
|
Widower |
8 (1.5%) |
|
Children number |
|
|
0 |
145 (26.9%) |
|
1-2 |
133 (24.7%) |
|
3 or more |
261 (48.4%)# |
|
Chronic diseases |
|
|
No diseases |
399 (74.0%)# |
|
Have diseases |
140 (26%) |
|
Diabetes |
28 (5.2%) |
|
Hypertension |
44 (8.2%) |
|
Obesity |
45 (8.3%) |
|
Respiratory diseases |
23 (4.3%) |
|
Work status |
|
|
Work away from the home |
187 (34.7%)# |
|
Work from home |
168 (31.2%) |
|
Not applicable |
184 (34.1%) |
Data are expressed as frequency (n). #Marked the prevalent group.
Marketing Habits of the Participants during the COVID-19 Pandemic
The findings revealed that 42.4% of the participants did not store additional food and were not concerned about food insecurity, whereas 34.6% of the participants went to store extra food and buy more than regular for fear of a shortage of food in the markets. Regarding the different ways of shopping during the pandemic, 34.5% of the participants relied on online shopping, while 43% preferred to shop from the markets. 62.9 % of the participants reported that they sanitize purchases before using them. According to the findings, 87.4 % of the participants did not change their meat-eating habits, while just 12.6 % of them planned to cut their meat consumption (Table 3).
Table 2. Nutritional habits and bodyweight variation of the participants during the COVID-19 pandemic
|
Character |
Frequency (%) |
|
Amount of water per day (glass) |
|
|
1-4 |
303 (56.2%)# |
|
5-7 |
148 (27.5%) |
|
≥ 8 |
88 (16.3%) |
|
Number of meals per day |
|
|
1-2 |
274 (50.8%)# |
|
3-4 |
250 (46.4%) |
|
> 5 |
15 (2.8%) |
|
Skip some meals |
|
|
Always |
111 (20.6%) |
|
Sometimes |
364 (67.5%)# |
|
Never |
64 (11.9%) |
|
The reason for skipping some daily meals |
|
|
Weight reduction |
131 (24.3%) |
|
Lack of time |
201 (37.3%)# |
|
Loss of appetite |
101 (18.7%) |
|
Reducing the amount of food eaten |
90 (16.7%) |
|
Fasting |
16 (3.0%) |
|
Type of meals per week |
|
|
Home made |
453 (84.0%)# |
|
Restaurants made |
50 (9.3%) |
|
Frozen (ready to eat) |
9 (1.7%) |
|
Fast food |
24 (4.5%) |
|
From restaurants dedicated to serving healthy meals |
3 (0.5%) |
|
Reason not to eat in restaurants |
|
|
Fear of pollution |
121 (22.5%) |
|
Rising prices |
177 (32.8%)# |
|
Low nutritional value |
95 (17.6%) |
|
Concentration on healthy food to post immunity |
146 (27.1%) |
|
Number of fast-food meals per week |
|
|
0 |
71 (13.2%) |
|
1-2 |
341 (63.3%)# |
|
3-4 |
105 (19.5%) |
|
5 or more |
22 (4.0%) |
|
Emotional eating |
|
|
Yes |
291 (54%)# |
|
No |
87 (16.1%) |
|
Sometimes |
161 (29.9%) |
|
Types of food most common in persons who experienced emotional eating |
|
|
Sugars |
200 (44.3%)# |
|
Chips and biscuits |
127 (28.1%) |
|
Pastries |
62 (13.7%) |
|
Nuts |
63 (13.9%) |
|
Bodyweight variation during COVID-19 pandemic |
|
|
Constant |
205 (38.0%) |
|
Increase |
237 (44.0%)# |
|
Decrease |
97 (18.0%) |
Data are expressed as frequency (n). #Marked the prevalent group.
Table 3. Marketing habits of the participants during the COVID-19 pandemic
|
Character |
Frequency (%) |
|
Storing extra amounts of food |
|
|
Yes |
187 (34.6%) |
|
No |
228 (42.4%)# |
|
Sometimes |
124 (23.0%) |
|
Online food shopping |
|
|
Yes |
186 (34.5%) |
|
No |
232 (43.0%)# |
|
Sometimes |
121 (22.5%) |
|
Sterilization of the purchased foods |
|
|
Yes |
339 (62.9%)# |
|
No |
65 (12.1%) |
|
Sometimes |
135 (25.0%) |
|
Change in meat purchase habits |
|
|
Yes |
68 (12.6%) |
|
No |
471 (87.4%)# |
Data are expressed as frequency (n). #Marked the prevalent group.
Daily Activities and Sleep Habits of the Participants During the COVID-19 Pandemic
The findings showed that 51% of the participants work or study for more than five hours per day, 46.6 percent undertake housework regularly, and 49.9% spend one to two hours per day in entertainment. About 36.2% of the participants exercised once to twice a week, 16.5% exercised three to four times a week, and 11.3% exercised daily, while 36% did not exercise at all. According to the findings, 43.6 percent of participants slept 7-9 hours per day, 64.9 percent of participants reported good sleep quality, and 41% did not suffer from anxiety due to the pandemic. As a result, 69.8% of the participants said they have a medium energy level during the day (Table 4).
Correlation between Increased Bodyweight during COVID-19 Pandemic and Emotional Eating, Physical Exercise, and Fast-Food Behavior
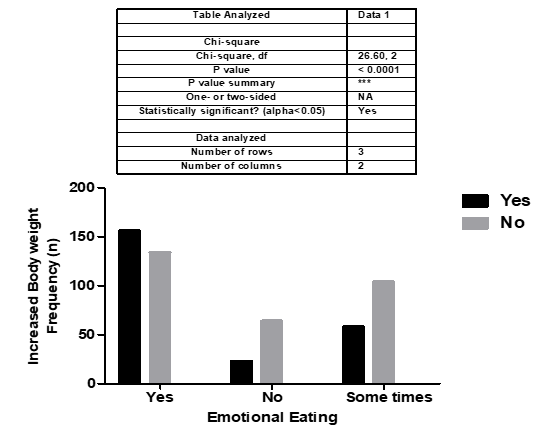
The chi-square correlation showed a strong correlation between emotional eating (p < 0.001) and increased body weight in the study participants. 44% of the participants reported increased body weight, and 54% exhibited emotional eating (Figure 1).
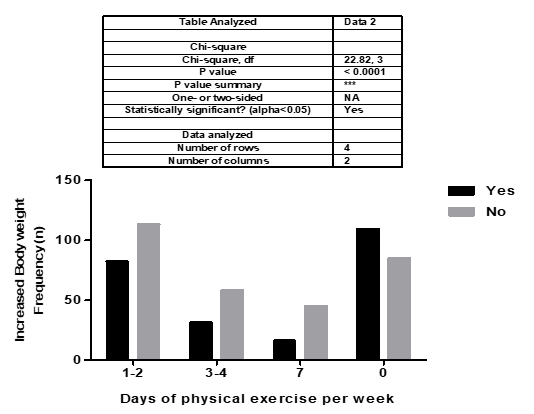
The chi-square correlation showed a strong correlation between physical exercise (p < 0.001) and increased body weight in the study participants. As 44% of the participants reported increased body weight and 36.2% exercised once to twice a week, 36% did not exercise at all (Figure 2).
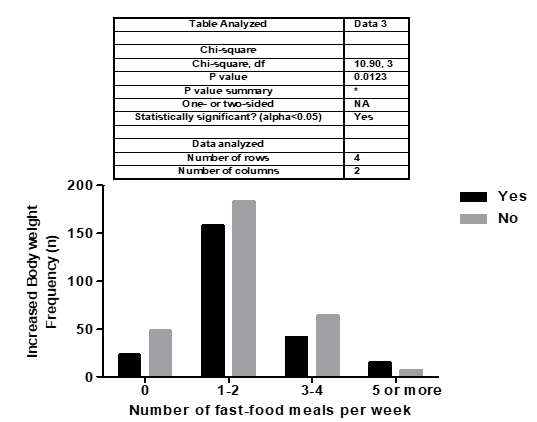
The chi-square correlation showed a significant correlation between the number of fast-food (p < 0.05) and increased body weight in the study participants. As 44% of the participants reported increased body weight and 23.5% eat fast food more than three times per week (Figure 3).
The current study was performed to discover modifications in lifestyle such as nutritional and marketing habits, daily activities, and sleep behavior in a sample collected from the western region, SA, during the COVID-19 quarantine time and explore their relationship with variations in body weight. The results revealed that most of the survey participants relied on home-cooked meals during the lockdown period, with the percentage of those eating out in restaurants declining. The demand for fast food also falls during the lockdown period. These findings are coherent with previous studies, which revealed that people are eating more home-cooked meals and less fast food during the pandemic (Górnicka et al., 2020; Abdulsalam et al., 2021; Ismail et al., 2021). The participants’ tendency to prefer home foods could be due to Coronavirus transmission through food, as food may be contaminated by vendors and handlers or through food bags and containers. Families may have changed their eating patterns to include more home-cooked meals and fewer restaurant meals to get healthier food. Households can benefit from programs that support home-cooked meals by including more healthful foods in their meals (Fertig et al., 2019).
Table 4. Daily activities and sleep habits of the participants during the COVID-19 pandemic
|
Character |
Frequency (%) |
|
Hours of work or study per day |
|
|
1-2 |
127 (23.6%) |
|
3-4 |
137 (25.4%) |
|
> 5 |
275 (51.0%)# |
|
Number of doing house cleaning per week |
|
|
Daily |
251 (46.6%)# |
|
1-3 |
207 (38.4%) |
|
4-5 |
20 (3.7%) |
|
Never |
61 (11.3%) |
|
Physical exercise per week |
|
|
1-2 |
195 (36.2%)# |
|
3-4 |
89 (16.5%) |
|
Daily |
61 (11.3%) |
|
Never |
194 (36.0%)# |
|
Hours of daily entertainment |
|
|
< 0.5 |
86 (16.0%) |
|
1-2 |
269 (49.9%)# |
|
3-4 |
135 (25%) |
|
5 or more |
49 (9.1%) |
|
Hours of sleep per day |
|
|
< 7 |
281 (52.1%)# |
|
7-9 |
235 (43.6%) |
|
> 9 |
23 (4.3%) |
|
Sleep quality |
|
|
Excellent |
69 (12.8%) |
|
Good |
350 (64.9%)# |
|
Bad |
120 (22.3%) |
|
Do you experience anxiety as a result of the pandemic? |
|
|
Yes |
159 (29.5%) |
|
No |
221 (41.0%)# |
|
Sometimes |
159 (29.5%) |
|
Energy level during the day |
|
|
High |
98 (18.2%) |
|
Medium |
376 (69.8%)# |
|
Low |
65 (12.0%) |
Data are expressed as frequency (n). #Marked the prevalent group.
 |
|
Figure 1. Chi-square correlation between increased body weight during COVID-19 pandemic and emotional eating behavior. Data are expressed as frequency (n). |
 |
|
Figure 2. Chi-square correlation between increased body weight during COVID-19 pandemic and physical exercise behavior. Data are expressed as frequency (n). |
 |
|
Figure 3. Chi-square correlation between increased body weight during COVID-19 pandemic and number of fast-food meals per week. Data are expressed as frequency (n). |
The present study results revealed that emotional ingestion was shown by about half of the participants, with the majority preferring sweets. The findings also showed that nearly the same percentage of participants reported an increase in body weight. There was a strong correlation between emotional eating and increased body weight. Similarly, excessive emotional eating was foretold by 365 Italian subjects during the lockdown period of the COVID-19 pandemic. Furthermore, they reported that a large BMI level was linked to increased emotional eating (Cecchetto et al., 2021).
In addition, a study involving 136 people in the United Kingdom found that when people are depressed, they have much more emotional eating cravings (McAtamney et al., 2021). Emotional eating was characterized as eating food in response to unpleasant emotions (for example, perceived stress) rather than internal hunger indicators (Shen et al., 2020). Sweet, fatty, and salty snack items were consumed in greater quantities by emotional eaters. According to many research, emotional eating has been linked to a higher BMI, stress, and sadness. In most studies, females were more affected by emotional eating, resulting in higher weight gain compared to males (Yau & Potenza 2013).
Stress causes physical and emotional weariness, which causes feeding and dietary habits to be disrupted (Albott et al., 2020; Rodgers et al., 2020; Shah et al., 2020). While acute stress usually inhibits eat desire, chronic stress causes the adrenal glands to secrete cortisol, which stimulates appetite, the incentive to eat, and the ingestion of energy-dense meals which are dense in calories, sweets, and fats (Born et al., 2010; Chao et al., 2017). Several hormones like leptin, ghrelin, and insulin are often impacted by persistent stress, and their quantities have a significant influence on satiety and eating desire and patterns (Yau & Potenza, 2013). Under stressful conditions, consumption of energy and fat-containing meals increases, and stress-induced cravings for “comfort food” that have large quantities of sugar and/or saturated fat are widespread (Lemmens et al., 2011; van Strien et al., 2019; Yunita et al., 2021). There is a strong link between stress and the consumption of soft drinks, salty snacks, sweet pastries, and fast meals. Similarly, there has been evidence of a detrimental relationship between stress and consuming fruit and veggies (Errisuriz et al., 2016; Tariq et al., 2019). Recent studies demonstrate that changes in dietary habits and food choices boosted the intake of macaroni, wheat, and frozen foods, while fresh food intake declined during the COVID-19 pandemic (Ashby, 2020; Bracale & Vaccaro, 2020; Di Renzo et al., 2020; Pellegrini et al., 2020).
These findings suggested that in Saudi Arabia, the individuals did not stockpile extra food and were not concerned about food insecurity. In line with these results, there was no panic buying in Qatar because the majority of the participants did not store food (Ben Hassen et al., 2020). The study’s findings also corroborate what was previously published by the Saudi Food & Drug Authority, 2020. According to this international investigation, the developing COVID-19 did not affect food availability or purchasing power in SA. The study was conducted during the global spread of the new Coronavirus pandemic, which forced countries to close, implement home quarantine, and impose social distancing measures, resulting in the closure of restaurants in many countries and causing people all over the world to stockpile basic foods and change how they choose and prepare foods. The survey included 37,714 persons from 38 nations, including 2,788 Saudi Arabians. The researchers came to the following conclusions about the rate of food consumption and food abundance: the unaffected nutritional habits of society in SA, and the lack of any effect on the rate of food storage, particularly meat, bread, flour, eggs, and milk, which confirms the lack of any impact on food abundance, purchasing power, and food storage. These results confirm the efforts made by the government of Saudi Arabia to achieve food security and food abundance during the pandemic.
The findings of this work revealed that the individuals’ weight gain during the lockdown period might have been caused by a reduction in exercise and physical activity. In line with our findings, a Saudi Arabian online survey of 1965 participants from May 11 to June 6, 2020, found that home quarantine had a detrimental impact on physical activity (Alfawaz et al., 2021; Taju et al., 2021). In addition, another study found that COVID-19 harmed physical activity, with 52 percent of participants reducing their activity, which was linked to considerable weight gain (Bakhsh et al., 2021). This finding revealed that as in other constrained conditions such as isolation could cause a significant fall in sports participation (Arries & Maposa, 2013; Belavý et al., 2013). Moreover, Al-Musharaf et al. (2021) revealed that during the COVID-19 lockdown period a significant proportion of particpants gained weight, the risk factors associated with weight gain were stress, sleep hours, and decline in physical activity. In a semi-structured interviews with 41 Saudi adults, most responses were marked by a high awareness about healthy eating. During the lockdown, physical activity declined, causing participants to become more stressed. The COVID-19 lockdown resulted in several changes in eating habits, including increased intake of snacks, sweets, fruits, vegetables, and home-cooked meals (Saaty & Aljadani, 2021). Recently, Alghamdi et al., (2022) reported that during COVID-19 quarantine, university students were under various types of stressors which might have affected their quality and quantity of sleep, and consequently, their quality of life.
CONCLUSION
The current findings revealed that most survey participants relied on home-cooked meals during the COVID-19 lockdown period. People in SA did not stockpile food and were unconcerned about food scarcity. Furthermore, almost half of the participants reported increased body weight gain, and emotional eating, with the majority favoring sweets. Weight gain may have been induced by a reduction in exercise and physical activity and increased emotional eating.
ACKNOWLEDGMENTS: The authors would like to thank all participants for their contribution in this study.
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: The objectives and procedures of the study were explained to the participants, and informed consent was obtained from all the participants.
Abdulsalam, N., Khateeb, N., Aljerbi, S., Alqumayzi, W., Balubaid, S., Almarghlani, A., Ayed, A. A., & Williams, L. L. (2021). Assessment of dietary habits and physical activity changes during the full COVID-19 curfew period and its effect on weight among adults in Jeddah, Saudi Arabia. International Journal of Environmental Research and Public Health, 18(16), 8580.
Albott, C., Wozniak, J., McGlinch, B., Wall, M., Gold, B., & Vinogradov, S. (2020). Battle Buddies: Rapid deployment of a psychological resilience intervention for health care workers during the coronavirus disease 2019 pandemic. Anesthesia and Analgesia, 131(1), 43-54.
Alfawaz, H., Amer, O., Aljumah, A., Aldisi, D., Enani, M., Aljohani, N., Alotaibi, N. H., lshingetti, N., Alomar, S. Y., Khattak, M. N. K., et al. (2021). Effects of home quarantine during COVID-19 lockdown on physical activity and dietary habits of adults in Saudi Arabia. Scientific Reports, 11(1), 5904.
Alghamdi, A. A., Alafif, N. O., BaHammam, A. S., Almuammar, M., Alharbi, N. S., Alhefdhi, N. A., Al-Musharaf, S., Al Ghamdi, K. S., AlYousif, G. F. & Al Muhanna, N. F. (2022). Nightmares’ Pattern and Predictors among a Saudi University Students during COVID-19 Pandemic. Journal of Environmental Research and Public Health, 19(3), 1776.
Al-Musharaf, S., Aljuraiban, G., Bogis, R., Alnafisah, R., Aldhwayan, M. & Tahrani, A. (2021). Lifestyle changes associated with COVID-19 quarantine among young Saudi women: A prospective study. PloS one, 16(4), e0250625.
Alzahrani, S., Saeedi, A., Baamer, M., Shalabi, A., & Alzahrani, A. (2020). Eating habits among medical students at King Abdulaziz University, Jeddah, Saudi Arabia. International Journal of General Medicine, 13, 77-88.
Arries, E. J., & Maposa, S. (2013). Cardiovascular risk factors among prisoners: an integrative review. Journal of Forensic Nursing, 9(1), 52-64.
Ashby, N. J. (2020). Impact of the COVID‐19 pandemic on unhealthy eating in populations with obesity. Obesity, 28(10), 1802-1805.
Bakhsh, M. A., Khawandanah, J., Naaman, R. K., & Alashmali, S. (2021). The impact of COVID-19 quarantine on dietary habits and physical activity in Saudi Arabia: A cross-sectional study. BMC Public Health, 21(1), 1-10.
Belavý, D., Gast, U., Daumer, M., Fomina, E., Rawer, R., Schießl, H., Schneider, S., Schubert, H., Soaz, C., & Felsenberg, D. (2013). Progressive adaptation in physical activity and neuromuscular performance during 520d confinement. PLoS One, 8(3), e60090.
Ben Hassen, T., El Bilali, H., & Allahyari, M. S. (2020). Impact of COVID-19 on food behavior and consumption in Qatar. Sustainability, 12(17), 6973.
Bhutani, S., & Cooper, J. A. (2020). COVID-19–related home confinement in adults: Weight gain risks and opportunities. Obesity, 28(9), 1576-1577.
Born, J., Lemmens, S., Rutters, F., Nieuwenhuizen, A., Formisano, E., Goebel, R. & Westerterp-Plantenga, M. S. (2010). Acute stress and food-related reward activation in the brain during food choice during eating in the absence of hunger. International Journal of Obesity, 34(1), 172-181.
Bracale, R., & Vaccaro, C. M. (2020). Changes in food choice following restrictive measures due to Covid-19. Nutrition, Metabolism and Cardiovascular Diseases, 30(9), 1423-1426.
Calder, P. C., Carr, A. C., Gombart, A. F., & Eggersdorfer, M. (2020). Optimal nutritional status for a well-functioning immune system is an important factor to protect against viral infections. Nutrients, 12(4), 1181.
Cecchetto, C., Aiello, M., Gentili, C., Ionta, S., & Osimo, S. A. (2021). Increased emotional eating during COVID-19 associated with lockdown, psychological and social distress. Appetite, 160, 105122.
Chao, A. M., Jastreboff, A. M., White, M. A., Grilo, C. M., & Sinha, R. (2017). Stress, cortisol, and other appetite‐related hormones: Prospective prediction of 6‐month changes in food cravings and weight. Obesity, 25(4), 713-720.
Di Renzo, L., Gualtieri, P., Pivari, F., Soldati, L., Attinà, A., Cinelli, G., Leggeri, C., Caparello, G., Barrea, L., Scerbo, F., et al., (2020). Eating habits and lifestyle changes during COVID-19 lockdown: an Italian survey. Journal of Translational Medicine, 18(1), 1-15.
Errisuriz, V. L., Pasch, K. E., & Perry, C. L. (2016). Perceived stress and dietary choices: The moderating role of stress management. Eating Behaviors, 22, 211-216.
Fertig, A. R., Loth, K. A., Trofholz, A. C., Tate, A. D., Miner, M., Neumark-Sztainer, D., & Berge, J. M. (2019). Compared to pre-prepared meals, fully and partly home-cooked meals in diverse families with young children are more likely to include nutritious ingredients. Journal of the Academy of Nutrition and Dietetics, 119(5), 818-830.
Galanakis, C. M., Aldawoud, T., Rizou, M., Rowan, N. J., & Ibrahim, S. A. (2020). Food ingredients and active compounds against the coronavirus disease (COVID-19) pandemic: A comprehensive review. Foods, 9(11), 1701.
Galli, F., Reglero, G., Bartolini, D., & Visioli, F. (2020). Better prepare for the next one. Lifestyle lessons from the COVID-19 pandemic. PharmaNutrition, 12, 100193.
Górnicka, M., Drywień, M. E., Zielinska, M. A., & Hamułka, J. (2020). Dietary and lifestyle changes during COVID-19 and the subsequent lockdowns among Polish adults: a cross-sectional online survey PLifeCOVID-19 study. Nutrients, 12(8), 2324.
He, M., Xian, Y., Lv, X., He, J., & Ren, Y. (2021). Changes in body weight, physical activity, and lifestyle during the semi-lockdown period after the outbreak of COVID-19 in China: an online survey. Disaster Medicine and Public Health Preparedness, 15(2), e23-e28.
Ismail, L., Osaili, T., Mohamad, M., Al Marzouqi, A., Jarrar, A. & Zampelas, A. (2021). Assessment of eating habits and lifestyle during the coronavirus 2019 pandemic in the Middle East and North Africa region: A cross-sectional study. British Journal of Nutrition, 126(5), 757-766.
Jansen, E. C., Prather, A., & Leung, C. W. (2020). Associations between sleep duration and dietary quality: results from a nationally-representative survey of US adults. Appetite, 153, 104748.
Lemmens, S. G., Rutters, F., Born, J. M., & Westerterp-Plantenga, M. S. (2011). Stress augments food ‘wanting’and energy intake in visceral overweight subjects in the absence of hunger. Physiology & Behavior, 103(2), 157-163.
Maggini, S., Pierre, A., & Calder, P. C. (2018). Immune function and micronutrient requirements change over the life course. Nutrients, 10(10), 1531.
McAtamney, K., Mantzios, M., Egan, H., & Wallis, D. J. (2021). Emotional eating during COVID-19 in the United Kingdom: Exploring the roles of alexithymia and emotion dysregulation. Appetite, 161, 105120.
Muscogiuri, G., Barrea, L., Savastano, S., & Colao, A. (2020). Nutritional recommendations for CoVID-19 quarantine. European Journal of Clinical Nutrition, 74(6), 850-851.
Obied, D. A., Alhamlan, F. S., Al-Qahtani, A. A., & Al-Ahdal, M. N. (2020). Containment of COVID-19: the unprecedented response of Saudi Arabia. The Journal of Infection in Developing Countries, 14(07), 699-706.
Park, S. H., Lee, E. J., & Chang, K. J. (2020). Dietary habits and snack consumption behaviors according to level of job stress among 20-to 30-year old office workers in the Seoul metropolitan area. Journal of the Korean Society of Food Culture, 35(2), 143-155.
Parmet, W. E., & Sinha, M. S. (2020). Covid-19—the law and limits of quarantine. New England Journal of Medicine, 382(15), e28.
Patton, A. P., & Hastings, M. H. (2018). The suprachiasmatic nucleus. Current Biology, 28(15), R816-R822.
Pellegrini, M., Ponzo, V., Rosato, R., Scumaci, E., Goitre, I., Benso, A., Belcastro, S., Crespi, C., De Michieli, F., Ghigo, E., et al. (2020). Changes in weight and nutritional habits in adults with obesity during the “lockdown” period caused by the COVID-19 virus emergency. Nutrients, 12(7), 2016.
Pokhrel, S., & Chhetri, R. (2021). A literature review on impact of COVID-19 pandemic on teaching and learning. Higher Education for the Future, 8(3), 234763112098348.
Reyes-Olavarría, D., Latorre-Román, P. Á., Guzmán-Guzmán, I. P., Jerez-Mayorga, D., Caamaño-Navarrete, F., & Delgado-Floody, P. (2020). Positive and negative changes in food habits, physical activity patterns, and weight status during COVID-19 confinement: associated factors in the Chilean population. International Journal of Environmental Research and Public Health, 17(15), 5431.
Rodgers, R., Lombardo, C., Cerolini, S., Franko, D., Omori, M., Fuller-Tyszkiewicz, M., Linardon, J. & Courtet, P. (2020). The impact of the COVID-19 pandemic on eating disorder risk and symptoms. International Journal of Eating Disorders, 53(7), 1166-1170.
Ruiz-Roso, M. B., Knott-Torcal, C., Matilla-Escalante, D. C., Garcimartín, A., Sampedro-Nuñez, M. A., Dávalos, A., & Marazuela, M. (2020). COVID-19 lockdown and changes of the dietary pattern and physical activity habits in a cohort of patients with type 2 diabetes mellitus. Nutrients, 12(8), 2327.
Saaty, A. H., & Aljadani, H. M. (2021). Investigating the influence of COVID-19 quarantine on health-related determinants among Saudi adults: A qualitative study. Pharmacophore, 12(3), 68-76.
Scarmozzino, F., & Visioli, F., (2020). COVID-19 and the subsequent lockdown modified dietary habits of almost half the population in an Italian sample. Foods, 9(5), 675.
Shah, M., Sachdeva, M., & Johnston, H. (2020). Eating disorders in the age of COVID-19. Psychiatry Research, 290, 113122.
Shen, W., Long, L. M., Shih, C. H., & Ludy, M. J. (2020). A humanities-based explanation for the effects of emotional eating and perceived stress on food choice motives during the COVID-19 pandemic. Nutrients, 12(9), 2712.
Sidor, A., & Rzymski, P. (2020). Dietary choices and habits during COVID-19 lockdown: experience from Poland. Nutrients, 12(6), 1657.
Taju, N. F. S., Ahmed, B. G., Abukhalid, N. H., Alsaikhan, A. S., Alhayyaf, H. H., Alotaibi, K. H., Alsahafi, A. S., Alotaibi, M. S., Alqahtani, F. T., Alanazi, A. F., et al. (2021). An overview on the role of MRI in diagnosis and management of berry aneurysm. World Journal of Environmental Biosciences, 10(3), 38-41. doi:10.51847/0hl1BHlLpm
Tariq, S., Tariq, S., & Tariq, S. (2019). Association of perceived stress with healthy and unhealthy food consumption among teenagers. The Journal of the Pakistan Medical Association, 69(12), 1817-1821.
van Strien, T., Gibson, E. L., Baños, R., Cebolla, A., & Winkens, L. H. (2019). Is comfort food actually comforting for emotional eaters? A (moderated) mediation analysis. Physiology & Behavior, 211, 112671.
Vieira, C. M., Franco, O. H., Restrepo, C. G., & Abel, T. (2020). COVID-19: The forgotten priorities of the pandemic. Maturitas, 136, 38-41.
WHO. (2020 a). World Health Organization. COVID-19 and food safety: Guidance for food businesses. World Health Organization.
WHO. (2020 b). World Health Organization/Europe. Physical activity - How to stay physically active during COVID-19 self-quarantine. World Health Organization. Available from: https://www.euro.who.int/en/health-topics/disease-prevention/physical-activity/news/news/2020/3/how-to-stay-physically-active-during-covid-19-self-quarantine
Yau, Y. H., & Potenza, M. N. (2013). Stress and eating behaviors. Minerva Endocrinologica, 38(3), 255-267.
Yunita, E. P., Suryanti, W. P., & Candradikusuma, D. (2021). New-onset type 2 DM risk in dyslipidemia and stroke patients due to simvastatin use. Journal of Advanced Pharmacy Education and Research, 11(3), 137-143. doi:10.51847/qvunlqV9fN