Improving the performance of any organization depends mainly on its organizational health. This descriptive-analytical and cross-sectional study aimed to investigate the relationship between managers' leadership styles and organizational health in Ahvaz teaching hospitals. The Hershey et al. and OHI scales for measuring leadership style and organizational health were distributed among 160 nurses working in five teaching hospitals in Ahvaz using the convenience cluster sampling method. The data correlation was analyzed using SPSS22. The organizational health level in Ahvaz hospitals was relatively good (149.60 ± 17.72). The predominant leadership styles in Ahvaz hospital managers were selling and telling styles. The findings of the study showed a weak positive correlation (r = 0.22) between selling style and organizational health and a weak negative correlation (r = -0.20) between delegating style and organizational health, both significant (P = 0.006 and P = 0.009, respectively). Besides, the telling leadership style had a significant positive correlation with institutional and managerial levels (institutional integrity and initiating structure dimensions), and the delegating leadership style had a noteworthy negative correlation with institutional and managerial levels (institutional integrity, initiating structure, and consideration dimensions). This study confirmed the positive relationship between telling leadership style and creating a healthy hospital environment, and the negative relationship between delegating leadership style and organizational health. However, comparing different leadership styles concerning organizational health requires further studies, especially in the hospital setting.
INTRODUCTION
An organization is a living organism that goes through stages, including health, illness, and death (Mosadeghrad & Esmaeili, 2017). The concept of organizational health was first introduced by Miles in 1969 (Miles, 1969). Organizational health includes a set of relatively stable organizational features. It indicates a situation beyond the short-term effectiveness of the organization (ZahedBabolan et al., 2008). Miles articulated these characteristics in meeting the basic needs, including, functional, survival, organizational growth, and development needs (Miles, 1969). A healthy organization can survive in a changing environment, continuously develop its capabilities and skills, and challenge problems (Toprak et al., 2015). It has a favorable climate and committed, conscientious, and motivated employees. Such an organization is agile, easily adapts itself to environmental changes, and continuously develops its capabilities (Mosadeghrad & Esmaeili, 2017). People are interested in working with this organization and are proud to be a part of it (Ansari et al., 2010).
A hospital’s organizational health is necessary for the effective and efficient achievement of the established goals, such as providing high-quality patient service (Mosadeghrad & Esmaeili, 2017). Improving organizational health has some positive effects on employees, such as improving work attitude (Ansari et al., 2010), organizational commitment (Jafari et al., 2012; Farzad et al., 2016), and organizational citizenship behavior (Nader et al., 2013), which will ultimately lead to their performance improvement. A favorable climate and employee motivation make healthy and dynamic hospitals more effective (Nader et al., 2013).
Several factors can be related to organizational health status, among which hospital managers’ leadership style is a matter that needs to be carefully considered (den Breejen-de Hooge et al., 2021; Losty & Bailey, 2021; Sansuwito et al., 2022). Although some researchers have challenged the importance of the leadership role in organizational performance (Meindl et al., 1985; Aldoory & Toth, 2004), others have concluded that organizational leadership is an important position and can play an imperative role in achieving organizational goals by creating an organizational climate affecting the employees’ attitude, motivation, and behavior (O'Reilly et al., 2010; Toprak et al., 2015; Ferramosca et al., 2021; Widianto, 2021). Managers playing the role of organizational leaders use different styles to guide human resources (Yusefi et al., 2014). According to situational leadership theory, leadership style emphasizes the combination of duty-oriented and behavior-oriented manner, which forms four main dimensions: telling, selling, participating, and delegating (Hersey et al., 1979). Some researchers believe that managers’ leadership style is one of the factors affecting organizational health and leads to organizational productivity (Nader et al., 2013; Ahmadi & Bazrafshan, 2014; AliNasab & Momayez, 2018) and therefore consider organizational health as one of the indicators of leadership effectiveness in the organization (Tsai, 2008).
This study aims to investigate the relationship between hospital managers’ leadership style and organizational health and is conducted based on the perception of the nurses working in teaching hospitals in Ahvaz in 2019. It seems that this study will help the existing literature by examining the leadership styles that are more correlated with creating organizational health.
MATERIALS AND METHODS
This cross-sectional descriptive-analytical study was conducted in 2019. The study population comprised all nurses working in teaching hospitals in Ahvaz, and the research sample included 160 nurses working in 5 teaching hospitals. The following formula was used to determine the sample size:
|
n=Z1-α2+Z1-β2W2+3 |
(1) |
The sample size was determined according to the previous studies’ findings, considering the 5% confidence level and 80% test power. Referring to the research environment in person, the researcher used the cluster sampling method to collect the data.
The data collection tool was a questionnaire consisting of three parts used after validity and reliability confirmation. The first part included demographic information, and in the second part, Hoy and Feldman’s Organizational Health Questionnaire (OHI) measured organizational health (Hoy & Fedman, 1987). There were 44 questions based on seven dimensions, including institutional integrity, principal influence, consideration, initiating structure, resource support, morale, and academic emphasis. It measured organizational health at three levels (institutional, managerial, and technical) based on a five-point Likert scale (always, often, sometimes, rarely, never). The scores ranging between 44-87, 88-131, 132-169, and 170-220 were considered low, normal, high, and very high organizational health, respectively. In the third part, a 12-item leadership style questionnaire was used. The questionnaire was based on the situational leadership theory by Hershey, Blanchard, and Neumeier. According to this theory, leadership style has four modes, including telling, selling, participating, and delegating (Hersey et al., 1979). In this questionnaire, leadership style was assessed based on the employees' opinions about their managers’ behavioral reactions in hypothetical situations.
Statistics such as mean, standard deviation, frequency distribution, and graphing were used for descriptive data analysis. The correlation between leadership style and organizational health was calculated using the Pearson correlation test with an alpha level of <0/05 and a 95% confidence interval using SPSS 22. The study noticed ethical considerations, including obtaining necessary permissions (approved code of ethics), the right of voluntary participation in the research, and using the data only for the study objectives.
RESULTS AND DISCUSSION
Table 1 provides the demographic data for the participants. The majority of nurses (46.3%) were between the ages of 20 and 30. There were 137 female nurses (85.6%), 86 unmarried nurses (53.8%), and 157 nurses (98.1%) with a bachelor's degree. Of these, 97.5% held nursing roles, 48 nurses worked in the emergency room (30%), 70.6% had 0–10 years of experience, and 34.4% had official employment positions.
Table 1. Study Variables
|
Percent |
Frequency |
Categories |
Variables |
|
13.8 |
22 |
R |
Hospital Labels |
|
12.5 |
20 |
B |
|
|
13.8 |
22 |
A |
|
|
33.1 |
53 |
G |
|
|
26.9 |
43 |
E |
|
|
85.6 |
137 |
Female |
Gender |
|
14.4 |
23 |
Male |
|
|
53.8 |
86 |
Single |
Marital Status |
|
46.3 |
74 |
Married |
|
|
98.1 |
157 |
BS |
Education |
|
1.9 |
3 |
MS and more |
|
|
9.4 |
15 |
Company |
Employment Scheme |
|
28.1 |
45 |
Contractual |
|
|
34.4 |
55 |
Official |
|
|
28.1 |
45 |
Others |
|
|
20.0 |
32 |
Surgery |
Ward |
|
18.1 |
29 |
Internal Medicine |
|
|
30.0 |
48 |
Emergency |
|
|
5.0 |
8 |
Pediatrics |
|
|
18.7 |
30 |
ICU |
|
|
2.5 |
4 |
CCU |
|
|
5.6 |
9 |
Psychiatry |
|
|
70.6 |
113 |
0-10 years |
Work Experiences |
|
27.5 |
44 |
11-20 years |
|
|
1.9 |
3 |
21-30 years |
|
|
46.3 |
74 |
20-30 years |
Age |
|
41.9 |
67 |
31-40 years |
|
|
10.6 |
17 |
41-50 years |
|
|
1.3 |
2 |
More than 51 years |
|
|
0.6 |
1 |
Head Nurse |
Organizational Position |
|
97.5 |
156 |
Nurse |
|
|
1.9 |
3 |
Nursing Intern |
|
|
8.8 |
14 |
1-10 |
Number of Beds |
|
53.8 |
86 |
11-20 |
|
|
12.5 |
20 |
21-30 |
|
|
19.4 |
31 |
31-40 |
|
|
5.0 |
8 |
41-50 |
|
|
0.6 |
1 |
51-60 |
|
|
100 |
160 |
|
Total |
Table 2 shows the mean, standard error, and standard deviation of organizational health scores and their dimensions. According to this table’s findings, the average score of the studied hospitals’ organizational health was 149.606 ( ± 17.72). This value is slightly above the average reference (3.40 of the average reference of 3 (P < 0.001)) (Table 3).
Table 2. Mean (Standard Deviation) of Organizational Health and its Dimensions and Levels by the Hospital.
|
Organizational Health |
Hospital Labels |
|||||
|
R |
E |
G |
B |
A |
Total |
|
|
Institutional Integrity |
21.23 ±2.99 |
22.30 ±3.77 |
21.02 ±3.43 |
22.25 ±3.93 |
22.00 ± 2.22 |
21.68 ±3.41 |
|
Principal Influence |
16.59 ±1.99 |
16.86 ±2.13 |
16.94 ±2.67 |
16.55 ±1.76 |
17.73 ±2.37 |
16.93 ±2.30 |
|
Consideration |
18.73 ±2.99 |
17.23 ±3.32 |
16.49 ±4.15 |
19.15 ±3.39 |
19.27 ±3.67 |
17.71 ±3.82 |
|
Initiating Structure |
21.50 ±2.58 |
21.37 ±3.01 |
19.13 ±4.40 |
21.55 ±2.54 |
22.14 ±3.03 |
20.77 ±3.60 |
|
Resource Support |
18.45 ±2.56 |
20.21 ±4.45 |
19.28 ±4.66 |
21.55 ±2.82 |
20.91 ±4.24 |
19.93 ±4.18 |
|
Morale |
26.18 ±2.80 |
26.67 ±4.24 |
26.00 ±4.48 |
26.00 ±2.58 |
28.09 ±5.14 |
26.49 ±4.14 |
|
Academic Emphasis |
25.09 ±3.01 |
25.79 ±3.90 |
25.64 ±5.43 |
27.20 ±2.67 |
27.73 ±5.23 |
26.09 ±4.48 |
|
Institutional Level |
21.23 ±2.99 |
22.40 ±3.63 |
19.51 ±4.23 |
22.25 ±3.93 |
21.95 ±2.21 |
21.20 ±3.82 |
|
Managerial Level |
75.27 ±7.41 |
75.67 ±8.73 |
71.85 ±11.35 |
78.80 ±6.87 |
79.91 ±10.80 |
75.33 ±9.94 |
|
Technical Level |
51.64 ±5.82 |
52.47 ±7.26 |
51.64 ±9.18 |
53.20 ±4.34 |
55.82 ±9.90 |
52.63 ±7.94 |
|
Total Organizational Health |
147.77 ±12.13 |
150.44 ±16.64 |
144.50 ±20.46 |
154.25 ±9.84 |
157.86 ±19.70 |
149.60 ±17.73 |
Table 3. The Hypothesis of a Significant Difference Between Organizational Health Means and Dimensions with the Reference Average
|
One-Sample Test |
||||||
|
|
Test Value = 3 |
|||||
|
t |
df |
P-value |
Mean Difference |
95% Confidence Interval of the Difference |
||
|
Lower |
Upper |
|||||
|
Institutional Integrity |
2.53 |
159 |
0.012* |
0.10 |
0.02 |
0.17 |
|
Principal Influence |
10.61 |
159 |
<0.001* |
0.39 |
0.31 |
0.46 |
|
Consideration |
8.98 |
159 |
<0.001* |
0.54 |
0.42 |
0.66 |
|
Initiating Structure |
20.26 |
159 |
<0.001* |
1.16 |
1.04 |
1.27 |
|
Resource Support |
14.92 |
159 |
<0.001* |
0.98 |
0.85 |
1.12 |
|
Morale |
-1.55 |
159 |
0.124 |
-0.06 |
-0.13 |
0.02 |
|
Academic Emphasis |
5.89 |
159 |
<0.001* |
0.26 |
0.17 |
0.35 |
|
Institutional Level |
0.66 |
159 |
0.508 |
0.03 |
-0.06 |
0.11 |
|
Managerial Level |
19.48 |
159 |
<0.001* |
0.77 |
0.69 |
0.84 |
|
Technical Level |
-11.74 |
159 |
<0.001* |
-0.37 |
-0.43 |
-0.31 |
|
Organizational Health |
12.56 |
159 |
<0.001* |
0.40 |
0.34 |
0.46 |
*P-value < 0.05
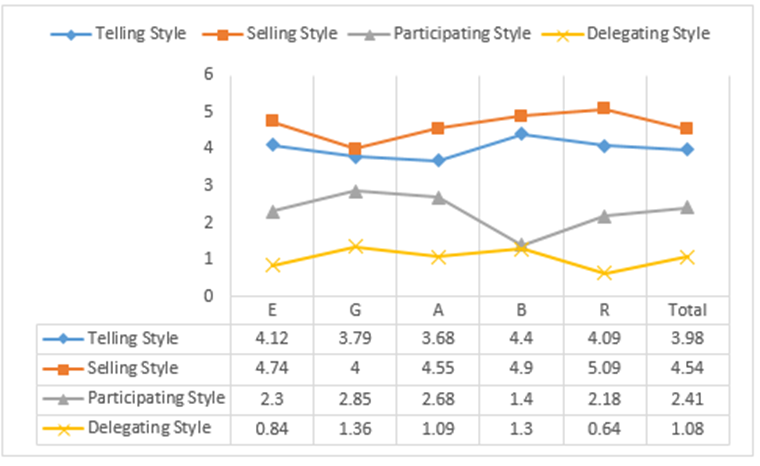
Figure 1 shows the mean scores of different types of leadership styles in the studied hospitals. According to the chart, the applied leadership styles in hospitals have mostly belonged to the selling (4.54 ± 1.74), telling (3.98 ± 1.85), participating (2.41 ± 1.68), and delegating (1.08 ± 1.45) styles, respectively.
|
|
|
Figure 1. Types of Leadership Styles in Teaching Hospitals in Ahvaz. |
Table 4 shows the relationship between different types of leadership styles and organizational health. Based on the table’s findings, there was a weak, positive (r = 0.22) and significant (P = 0.006) correlation between telling leadership style and organizational health. The findings also indicate a weak, inverse (r = -0.20) and significant (P = 0.009) correlation between delegating leadership style and organizational health. At the same time, no significant relationship was observed between selling and participating styles and organizational health.
Table 4. Relationship Between Different Types of Leadership Styles and Organizational Health (Levels and Dimensions).
|
Organizational Health |
|
Leadership Styles |
|||
|
|
Telling Style |
Selling Style |
Participating Style |
Delegating Style |
|
|
Institutional Integrity |
Pearson correlation |
0.26 |
-0.02 |
-0.02 |
-0.32 |
|
P-value |
0.001* |
0.823 |
0.771 |
< 0.001* |
|
|
Principal Influence |
Pearson correlation |
0.06 |
-0.10 |
0.06 |
-0.04 |
|
P-value |
0.443 |
0.190 |
0.452 |
0.605 |
|
|
Consideration |
Pearson correlation |
0.06 |
0.06 |
0.02 |
-0.18 |
|
P-value |
0.472 |
0.468 |
0.782 |
0.020* |
|
|
Initiating Structure |
Pearson correlation |
0.20 |
0.16 |
-0.18 |
-0.34 |
|
P-value |
0.010* |
0.047* |
0.023* |
< 0.001* |
|
|
Resource Support |
Pearson correlation |
0.15 |
-0.07 |
-0.04 |
-0.06 |
|
P-value |
0.060 |
0.400 |
0.643 |
0.493 |
|
|
Morale |
Pearson correlation |
0.12 |
-0.07 |
-0.05 |
-0.01 |
|
P-value |
0.140 |
0.370 |
0.542 |
0.911 |
|
|
Academic Emphasis |
Pearson correlation |
0.10 |
-0.09 |
0.09 |
-0.03 |
|
P-value |
0.219 |
0.235 |
0.266 |
0.702 |
|
|
Institutional Level |
Pearson correlation |
0.20 |
0.06 |
-0.06 |
-0.32 |
|
P-value |
0.009* |
0.419 |
0.467 |
< 0.001* |
|
|
Managerial Level |
Pearson correlation |
0.19 |
0.03 |
-0.08 |
-0.25 |
|
P-value |
0.018* |
0.697 |
0.321 |
0.001* |
|
|
Technical Level |
Pearson correlation |
0.12 |
-0.09 |
0.01 |
-0.02 |
|
P-value |
0.132 |
0.258 |
0.942 |
0.843 |
|
|
Organizational Health |
Pearson correlation |
0.22 |
-0.03 |
-0.04 |
-0.20 |
|
P-value |
0.006* |
0.703 |
0.590 |
0.009* |
|
*P-value < 0.05
According to the organizational health findings, the hospitals under study were able to sustain survival and environmental adaptability at a level that was relatively higher than the conceptual average, which is desired. While the technical level of organizational health was below average, the management and institutional levels were above average. At the same time, the highest rank was held by the management level. The construction and resource support aspects had the best status, according to the study's conclusions. When the hospitals under study placed a strong emphasis on following the rules and regulations in the interactions between management and staff, the construction component had a suitable status. Additionally, the resource support status showed that the hospital and its personnel were providing good supplies and equipment for effective care (Hoy & Fedman, 1987).
According to the findings, the institutional integrity dimension was the lowest in status. Institutional integrity demonstrates the ability to adapt to the environment and destructive environmental factors successfully. An unhealthy institutional integrity status shows managers’ poor performance in adapting to their environment and their failure in preventing the interference of personal and unscientific tastes inconsistent with the hospital's environmental conditions during hospital planning. Barati's study showed a significant relationship between institutional integrity and some hospital performance indicators (Marani et al., 2011), and Sadeghi's study indicated a strong, positive, and significant relationship between the dimension and organizational effectiveness (Sadeghi & Alavi, 2014). Therefore, planning to improve institutional integrity, which is considered the studied hospitals’ weakness, seems essential. Hospital managers should avoid hospital independence, external pressures, and unreasonable demands from staff and reduce hospital vulnerability to destructive environmental forces. On the other hand, institutional integrity is identified as one of the most influential factors affecting the employees’ organizational commitment, especially in professional settings (Nasiripour et al., 2011). Given that most educational hospitals have a high degree of professionalism, institutional integrity improvement planning is of great importance. Thus, corrective actions in this area are recommended. Managers' indifference to unreasonable pressures outside the hospital and setting some limits for outside influences can be a solution. Strengthening hospital managers’ perceptual skills and improving their performance in strategic thinking, strategic evaluation, and analysis of hospital situations can be useful, too. Furthermore, having a philosophical mindset can enable managers to deal with problems logically and correctly (Nazem & Sedghi Boukany, 2007), be safe from narrow-mindedness, self-centeredness, and one-sidedness under environmental pressures, and make rational and comprehensive decisions. The good status of the construction dimension compared with the undesirable status of the institutional integrity and the significant difference between them reinforces the hypothesis that the general positive status of organizational health could result from administrative control and supervision. In this regard, necessary care should be taken to transfer control and monitoring programs from negative to positive mode, and decisions should be made according to the principles of rationalism and participation to the possible extent.
In general, although the hospitals’ organizational health was relatively higher than the reference average, it requires balanced and comprehensive attention to all its dimensions and levels in the hospitals. A considerable part of the hospitals’ organizational health has been provided by structural and functional dimensions (construction and resource support dimensions), which belong to the administrative level. In the long term, for instance, resource limits will cause major shocks to the hospitals' performance if this uneven position persists, particularly during times of crisis. It will reduce hospital resilience to a potential crisis. As long as the hospital is exposed to fixed environments, it might not happen in the near future. Organizations operating in dynamic environments, like educational hospitals, are always subject to a variety of environmental factors. They will progressively deteriorate if their companies are unable to react to the situation fast and flexibly. Therefore, special attention must be paid to the institutional level and institutional integrity.
Thus, in order to promote hospital sustainability in the face of environmental unpredictability, attention to organizational health and its levels is suggested. It is critical at the institutional level and may be met by hiring skilled managers with management and leadership knowledge and abilities, as well as prioritizing these efforts within hospital organizational change and improvement programs.
In general, leadership style, or how a leader manages organizational processes, is considered an influential resource in creating organizational health in the workplace (Nader et al., 2013). It can be used as an inhibiting or facilitating factor for developing organizational health. Riley believes in the critical role of leadership in implementing organizational strategies that can help create a good organizational climate to form an excellent organizational environment (O'Reilly et al., 2010). When a leader affects the employees, inspires them, and motivates them to focus on the organization's goals, the hospital will have a better chance of surviving in a rapidly changing environment and a more remarkable ability to challenge the problems ahead naturally. However, available findings regarding the relationship between different types of leadership styles and organizational health seem contradictory.
The findings showed a significant positive correlation between the telling leadership style and organizational health, according to which any improvement or weakness in the telling leadership style would increase or decrease the hospitals’ organizational health. In addition, no significant relationship was observed between selling and participating styles and organizational health. The relationship between telling leadership style and organizational health could be partially justified based on the situational leadership theory. Thus, due to the participants’ little work experience, the telling style could have a positive relationship with creating organizational health. In the situational leadership theory, it is recommended to choose the appropriate leadership style according to the employees’ characteristics. However, it cannot be concluded that the Telling leadership style will lead to organizational health strengthening in any situation and with any employees. In some situations, the participating leadership style will lead to improved organizational health by facilitating continuous communication between employees and managers (Jafari et al., 2012).
This study showed a significant negative correlation between the delegating leadership style and organizational health. Any improvement or weakness in the delegating leadership style would have an opposite effect on hospital organizational health changes. No evidence was found to compare this dimension. Most previous studies have focused on the relationship between transformational and transactional leadership styles and organizational health. Toprak et al., Rastegar et al., and Korkmaz et al. reported the positive relationship between transformational leadership style and creating a healthy organization (Korkmaz, 2007; Toprak et al., 2015; Rastegar et al., 2019). Transformational leaders use intellectual stimulation to challenge employees’ thoughts and creativity and increase their knowledge, which increases employees' intrinsic motivation to create a healthy organization. As a result, these organizations’ employees will gain more tolerance and problem-solving power in the face of organizational challenges and crises (Korkmaz, 2007; Rastegar et al., 2019; Hussain & Khayat, 2021; Ishii et al., 2021; Martinussen & Davidsen, 2021). However, there are contradictory results. One study in Ilam showed the relationship between transactional leadership styles and organizational health (Nekoei Moghaddam et al., 2013). The study findings regarding the correlation strength among organizational health levels showed the highest correlation (negative) between delegating leadership style and institutional and managerial levels. This means that managers’ delegating leadership style led to reduced organizational health because of its negative relationship with institutional and managerial levels (Abbas et al., 2023; Ghanizadeh et al., 2023; Nurcahyo et al., 2023). The delegating style also had the most negative correlation with the initiating structure and institutional integrity dimensions. Secondly, the strongest correlation was observed between telling leadership style and institutional and managerial levels. When managers used the telling leadership style in dealing with hospital staff, the organizational health increased due to the positive correlation with institutional and managerial levels. The noteworthy point is the lack of correlation between the Telling style and technical level and its dimensions, that is, morale and academic emphasis. Taghi-Nasab et al. believed that the use of autocratic leadership styles could lead to mistrust and reduced employee’ morale in the long run, even if they were useful in the short term (Taghi Nasab et al., 2009). Considering the moral dimension, the present study showed a bad status and therefore is in line with Taghi-Nasab's findings. The telling leadership style also had the most positive correlation with the dimensions of institutional integrity and initiating structures. In this study, no relationship was found between any of the leadership styles, resource support, and principal influence, implying that there was no relationship between leadership style and the technical level of organizational health.
In general, it is concluded that what makes a leadership style implementation appropriate to improve organizational health is the organization’s environmental conditions and requirements. At present, due to the shortage of studies comparing different types of leadership styles and their relationship with organizational health (Taghi Nasab et al., 2009; AliNasab & Momayez, 2018), further studies are needed on the role of the factors such as leadership styles on organizational health, especially in hospital settings.
The capacity of hospital managers to establish a positive work atmosphere is proposed as a crucial metric for assessing their effectiveness. Constant attention to hospital levels and frequent information gathering regarding the health of the organization might also result from it. In order to improve the existing situation, a group of top hospital and university administrators might use this diagnostic instrument to determine the best leadership style based on its relationship to organizational health. Therefore, it is recommended that while arranging hospital managers' in-service training, senior management groups stress the development of suitable leadership styles and promote the use of appropriate leadership styles depending on the circumstances.
CONCLUSION
In conclusion, regardless of the discussed relationship between leadership styles and organizational health, the current hospital managers’ leadership styles have not led to increased hospital abilities to adapt to the environment to preserve the unity, coherence, and integrity of their training and treatment programs (the Institutional Integrity dimension) and improve their mutual trust of the employees in the organization (the morale dimension). The main influential feature of the current leadership style has been the organization’s internal supervision (the managerial level). Given that different situations require appropriate leadership practices, it is suggested that managers take into account the weaknesses of their current leadership styles by considering organizational health findings as one of the indicators of situation assessment and repair and adjust their guiding and supportive degrees according to the situation.
One limitation of this study is the reliance on self-expression tools because the individuals were likely not to respond accurately to the items. Also, the results can only be generalized to the research environment, so similar studies in other environments are recommended. In this study, organizational health levels were evaluated based on Hoy and Feldman’s classification. Evaluating other aspects of organizational health, such as ethics, creativity and innovation, planning, coherence, and integration, is suggested in future studies using other tools.
ACKNOWLEDGMENTS: None
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: The present study was financially supported by the Student Research Committee of Ahvaz Jundishapur University of Medical Sciences (98s50).
ETHICS STATEMENT: This study has been approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1398.364).
Abbas, K. S., Hasan, A. S., & Tareq, N. L. (2023). Assessment of the impact of different rheumatoid arthritis stages on the quality of life of a sample of Iraqi patients. Journal of Advanced Pharmacy Education and Research, 13(1), 122-126.
Ahmadi, E., & Bazrafshan, A. A. (2014). Relationship management styles to organizational health and job stress. Journal of New Approaches in Educational Administration, 5(2), 73-90.
Aldoory, L., & Toth, E. (2004). Leadership and gender in public relations: Perceived effectiveness of transformational and transactional leadership styles. Journal of Public Relations Research, 16(2), 157-183.
AliNasab, Z., & Momayez, S. (2018). The role of social capital, organizational justice and organizational citizenship behavior in predicting organizational health. Quarterly Journal of Nursing Management, 7(2), 27-36.
Ansari, M., Ostadi, H., & Javeri, F. (2010). The relationship between organizational health and positive attitudes of the staff in the offices of the provincial tax Isfahan. Journal of Tax, 6(54), 41-65.
den Breejen-de Hooge, L. E., van Os-Medendorp, H., & Hafsteinsdóttir, T. B. (2021). Is leadership of nurses associated with nurse-reported quality of care? A cross-sectional survey. Journal of Research in Nursing, 26(1-2), 118-132. doi:10.1177/1744987120976176
Farzad, M., Arab, M., & Ganji, H. (2016). Relationship between organizational health and organizational commitment in the central headquarters' staff of Zabol University of Medical Sciences, 2014. International Journal of Advanced Biotechnology and Research, 7, 2055-2060.
Ferramosca, F. M. P., Filomeno, L., Gualandi, R., Tartaglini, D., & Ivziku, D. (2021). The role of the leader on the nurses perception of work well-being. Professioni Infermieristiche, 74(4), 266-266.
Ghanizadeh, S. M., Mohammadi, M. A., Dadkhah, B., Raisi, L., & Mozaffari, N. (2023). Parenting stress and social support in mothers of children with disability in Ardabil, 2020. Journal of Advanced Pharmacy Education and Research, 13(1), 105-110.
Hersey, P., Blanchard, K. H., & Natemeyer, W. E. (1979). Situational leadership, perception, and the impact of power. Group & Organization Studies, 4(4), 418-428.
Hoy, W. K., & Fedman, J. A. (1987). Organizational health: The concept and its measure. Journal of research and Development in Education, 20(4), 30-37.
Hussain, M. K., & Khayat, R. A. M. (2021). The impact of transformational leadership on job satisfaction and organisational commitment among hospital staff: A systematic review. Journal of Health Management, 23(4), 614-630. doi:10.1177/09720634211050463
Ishii, K., Takemura, Y., & Ichikawa, N. (2021). Relationships between the components of nurse managers’ transformational leadership and organisational learning subprocesses in a hospital ward: A cross‐sectional study. Journal of Nursing Management, 29(4), 672-680. doi:10.1111/jonm.13203
Jafari, H., Mohammadian, M., & Hossein, P. D. (2012). Organizational health and its relation to organizational commitment in personnel of selected teaching hospitals affiliated with Ahvaz Jundishapur University of Medical Sciences: 2011. Jundishapur Journal of Health Sciences, 4(1), 41-48.
Korkmaz, M. (2007). The effects of leadership styles on organizational health. Educational Research Quarterly, 30(3), 23-55.
Losty, L. S., & Bailey, K. D. (2021). Leading through chaos: Perspectives from nurse executives. Nursing Administration Quarterly, 45(2), 118-125. doi:10.1097/NAQ.0000000000000456
Marani, A. B., Haghani, H., Mohammadi, R., Moradi, F., Rouhani, B., Torsaki, M., & Khodayari, R. (2011). The Relationship between Organizational Health and Performance Indicators of Health Care in Teaching Hospitals Affiliated to Tehran University of Medical Sciences: 2011. Journal of Health Administration, 14(46), 31-38.
Martinussen, P. E., & Davidsen, T. (2021). ‘Professional-supportive’ versus ‘economic-operational’ management: the relationship between leadership style and hospital physicians’ organisational climate. BMC Health Services Research, 21(1), 1-11. doi:10.1186/s12913-021-06760-2
Meindl, J. R., Ehrlich, S. B., & Dukerich, J. M. (1985). The romance of leadership. Administrative Science Quarterly, 30(1), 78-102.
Miles, M. B. (1969). Planned change and organizational health: Figure and ground. Organizations and Human Behavior, 375-391.
Mosadeghrad, A. M., & Esmaeili, M. (2017). A survey of organizational health in university hospitals of Isfahan. Health-Based Research, 2(4), 329-344.
Nader, K., Lida, S., Somaye, Y., Ebrahim, J. P., Taha, N., Narges, R., & Tayebe, M. (2013). The relationship between organizational health and organizational citizenship behavior in hospitals affiliated to Tehran university of medical sciences in 2010. Payavard Salamat, 6(6), 412-422.
Nasiripour, A. A., Alimohammadzadeh, K. H., Raeissi, P., & Jafari, M. (2011). The relationship between organizational safety culture and organizational commitment: A Case Study of Islamic Azad University, Science and Research. Journal of Healthcare Management, 3(1), 49-57.
Nazem, F., & Sedghi Boukany, N. (2007). The relationship between the emotional intelligence and philosophic mindeness of managers and organizational health. Journal of Thought & Behavior in Clinical Psychology, 1(2), 68-75.
Nekoei Moghaddam, M., Shokouhi, I., Baneshi, M. R., Nakhaei, N., & Afshar, Z. (2013). The relationship between leadership style and job satisfaction: A study on health care networks staff in Kerman University of medical sciences in 2011. Health and Development Journal, 2(1), 65-73.
Nurcahyo, H., Riyanta, A. B., Febriyanti, R., Sutanto, H., & Herdwiani, W. (2023). Hypolipidemic activity of Ceciwis ethanol extract on wistar rats induced by high fat in vivo. Journal of Advanced Pharmacy Education and Research, 13(1), 100-104.
O'Reilly, C. A., Caldwell, D. F., Chatman, J. A., Lapiz, M., & Self, W. (2010). How leadership matters: The effects of leaders' alignment on strategy implementation. The Leadership Quarterly, 21(1), 104-113.
Rastegar, A., Seif, M. H., Ardekani, Z. F., & Tajvaran, M. (2019). The relationship of transformational leadership style with bullying at work with regard to the mediating role of organizational health among employees of Shiraz university of medical sciences. Journal of Payavard Salamat, 13(4), 269-280.
Sadeghi, N., & Alavi, A. (2014). Relation of organizational health indicators and organizational effectiveness in health system. Health System Research Journal, 10(3), 548-557.
Sansuwito, T. B., Prasath, R., Novera, M., Sarli, D., Poddar, S., & Ariani, N. (2022). The effect of leadership styles on nurse performances and job satisfaction among nurses in Dumai public hospital: Technological innovation as mediator. Malaysian Journal of Medicine and Health Sciences, 18, 229-234.
Taghi Nasab, A., Pardakhtchi, M. H., & Ghahremani, M. (2009). Relationship of leadership style and organizational health in secondary schools. Journal of Management and Planning In Educational System, 2(1), 42-54.
Toprak, M., Inandi, B., & Colak, A. L. (2015). Do leadership styles influence organizational health? A study in educational organizations. International Journal of Educational Methodology, 1(1), 19-26.
Tsai, C. W. (2008). Leadership style and employee's job satisfaction in international tourist hotels. Advances in Culture, Tourism and Hospitality Research, 2(2), 293-332.
Widianto, S. (2021). Empowering leadership to performance excellence: The role of knowledge sharing and self-efficacy. International Journal of Business Excellence, 23(3), 297-311. doi:10.1504/IJBEX.2021.113701
Yusefi, A., Jabbari, A., Koushki, J., & Heidari, A. (2014). The relationship between personality type and leadership style of managers in educational hospitals of Shiraz University of Medical Sciences. Health and Development Journal, 3(1), 84-93.
ZahedBabolan, A., Asgarian, M., Behrangi, M., & Naderi, E. (2008). The relationship between school organizational health and organizational commitment of teachers in boy's high school in Ardabil province. Journal of Educational Studies and Psychology, 148(9), 127-148.